





How the Patient Found the Practice
Marianne was referred by a long-time patient and friend who had been receiving care at the practice for several years.
With trust already established through that connection, Marianne arrived with hope—and a broken front tooth.
Initial Condition & Life Before Treatment
Tooth #8 had a long history.
Years earlier, trauma led to a root canal. Over time, the tooth had discolored, though it remained functional.
Seeking to improve her smile, Marianne had internal whitening performed by an endodontist. However, just three months after that procedure, the tooth’s crown fractured spontaneously.
This sudden break left Marianne in both a physically and emotionally difficult position.
Her central front tooth—a focal point of her smile—was deemed non-restorable, and the idea of a visible prosthetic or complex replacement filled her with concern.
First Appointment & Discovery
At her first appointment, a thorough clinical exam and X-rays revealed there wasn’t enough remaining structure to support a lasting restoration.
The verdict was clear: the tooth could not be saved.
A follow-up with her restorative dentist confirmed that the best course of action was to extract the tooth and move toward implant replacement.
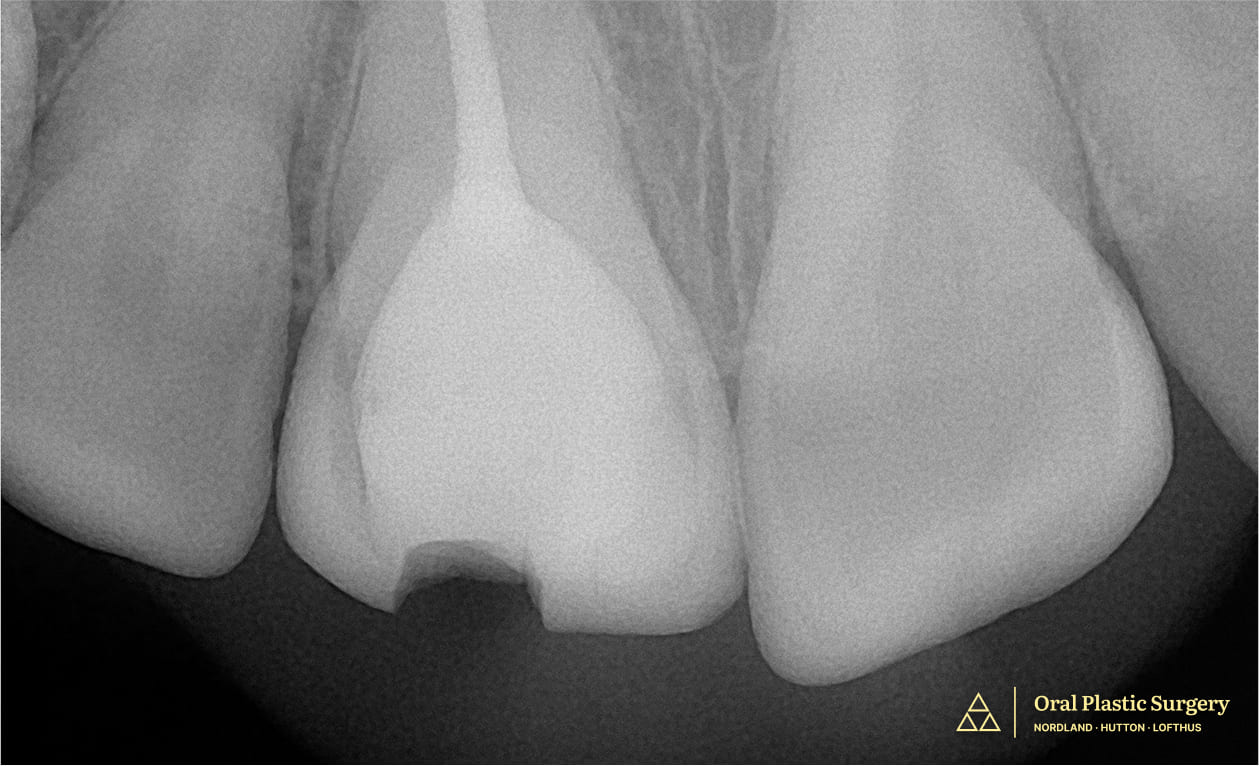
Showing a large filling and minimal natural structure, making the tooth non-restorable.
Why This Case Required Advanced Expertise
This wasn’t just about replacing a tooth—it was about restoring harmony, function, and esthetics in one of the most visible areas of the smile.
The patient also had specific requests: she did not want donor-derived (allograft) or animal-based (xenograft) materials used.
Instead, the team would need to rely entirely on her own tissue to rebuild the site and support an implant. This, combined with the need for esthetic excellence, required careful digital planning, precision surgery, and interdisciplinary collaboration.
Treatment Plan & Approach
To begin, a 3D X-ray was taken to digitally map the site and guide the surgical plan. The fractured tooth was gently extracted, and an implant was placed immediately.
A free gingival graft was also performed at the time of extraction.
In place of donor or animal grafts, the patient’s own bone—harvested from a nearby tori—was used to support the implant.
A small blood sample was drawn and processed into a healing membrane called Leukocyte- and Platelet-Rich Fibrin (L-PRF), which was applied to enhance recovery.
To ensure esthetics during healing, an Essix retainer with a temporary tooth was provided, allowing Marianne to maintain a natural-looking smile throughout her Invisalign treatment.

The ovate pontic on the Essix retainer helped shape the gum tissue, creating a natural-looking emergence profile.
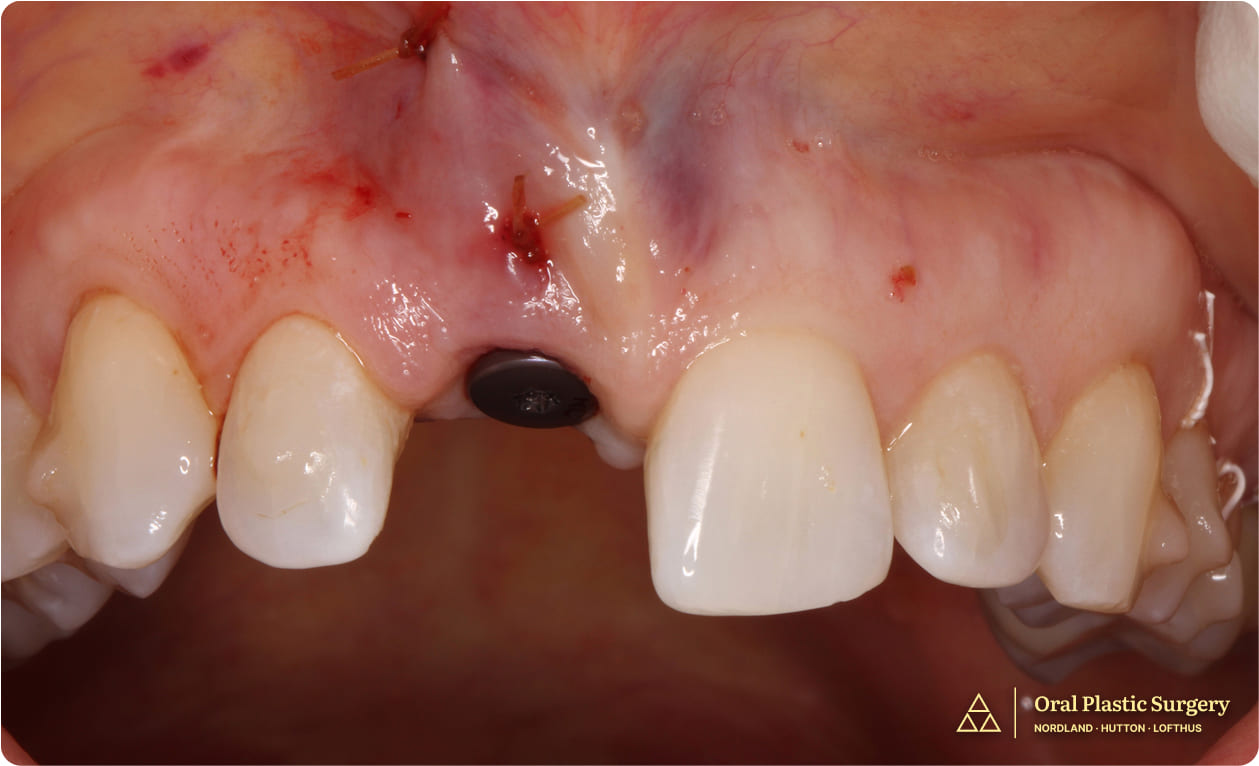
The implant was uncovered, a healing abutment was placed, and a ridge augmentation was performed to improve the gingiva contour.
Case Progression & Key Milestones
Later in the healing process, a ridge augmentation was performed at the time of implant uncovering to refine the soft tissue contours and improve the emergence profile.
The coordination between surgical and restorative teams ensured that each phase built seamlessly on the last, culminating in a result that was both functional and beautiful.
Outcome
Thanks to Dr. Hutton’s expertise, the implant achieved excellent stability and integration, with no complications.
Healing was smooth, and the use of autogenous tissue supported robust soft tissue health.
Because of the careful implant placement and ridge augmentation, the final crown mimicked the natural tooth in both shape and gum contour. The gumline emerged naturally around the new tooth, blending flawlessly with adjacent teeth.
Marianne expressed deep satisfaction with the outcome.
The use of her own tissue and a treatment process grounded in trust, collaboration, and precision helped restore not just her tooth but also her confidence and peace of mind.
Trust your smile to specialists who put patients first, with minimally invasive solutions designed to last.

Tooth #8 shows a visible fracture, indicating structural compromise and the need for further evaluation and treatment

Showing the completed restoration with a natural and seamless appearance
Clinical Notes for Referring Doctors
This case demonstrates the successful management of a fractured, non-restorable maxillary central incisor using immediate implant placement, autogenous bone harvesting, and soft tissue augmentation with L-PRF membranes.
No allografts or xenografts were used, as per the patient’s request. A second-stage ridge augmentation enhanced soft tissue contour and esthetics.
Coordination between the surgical and restorative teams ensured ideal outcomes. Dr. Hutton welcomes referrals for esthetic zone cases requiring biologically conservative and technically demanding implant reconstruction.





